Daniel Du, Applied Science
Abstract
This research paper presents the design and development of an emergency oxygen delivery device using the Max30100 sensor and Arduino Uno microcontroller. The device will provide oxygen therapy to victims in emergencies. It is portable, affordable, and easy to use, making it ideal in a resource limited setting. The study and experiments test the device’s accuracy. The de- vice’s accuracy significantly improved after implementing various algorithms: moving average, low pass, Kalman filter, and wavelet transform. The device operates based on the readings pro- vided by the MAX30100 sensor, which continuously monitors the victim’s blood oxygen level. The device can improve the quality of care for patients in emergencies.
Introduction
Oxygen therapy is an essential medical intervention for patients with low blood oxygen levels. It is commonly used in emergencies such as heart attacks, asthma, and respiratory failure. (Kane et al. 2013) Oxygen therapy aims to increase the oxygen supply to the body, improving the patient’s oxygen saturation levels and preventing further damage to the body.
Pulse oximetry is a non invasive method used to measure the oxygen saturation level of the blood. It uses a sensor that measures the absorption of light by the blood. The Max30100 sensor measures the patient’s oxygen saturation level and heart rate. It is a low cost and compact sensor. Previous studies have shown that the Max30100 sensor can be integrated with the Arduino micro- controller to develop medical devices for oxygen therapy. (Bhuyan and Sarder 2011). The Arduino microcontroller can be programmed to control oxygen delivery to the patient based on the oxygen saturation level measured by the Max30100 sensor.
Despite the availability of oxygen therapy devices, some limitations still need to be ad- dressed. The existing devices are often bulky, expensive, and require specialized training. These limitations make providing oxygen therapy in emergencies difficult, especially in resource limited settings. In the case of emergencies, such as sudden cardiac arrest, oxygen therapy will be effective if started shortly after the stroke and can prolong the need for neuroprotective drugs. (Singhal 2007). A study done at the Medical Research Institute of New Zealand compares the use of liberal and conservative oxygen therapy. They found that conservative oxygen therapy, which refers to providing the minimum amount of supplemental oxygen to patients, often targeting 90-94% oxy- gen saturation levels, had a significantly lower mortality rate. (Young et al. 2020)
With the device that this study presents, the user must strap on the oxygen mask and follow its instructions. The Arduino microcontroller is programmed to analyze the data from the MAX30100 sensor. The device can potentially improve the quality of care for patients in emer- gencies, and further studies are needed to evaluate its effectiveness in different clinical settings. The device has an oxygen delivery. Oxygen can be delivered through low flow systems; however, there can be side effects and complications with oxygen therapy. (Mach et al. 2011)
Materials and Methods
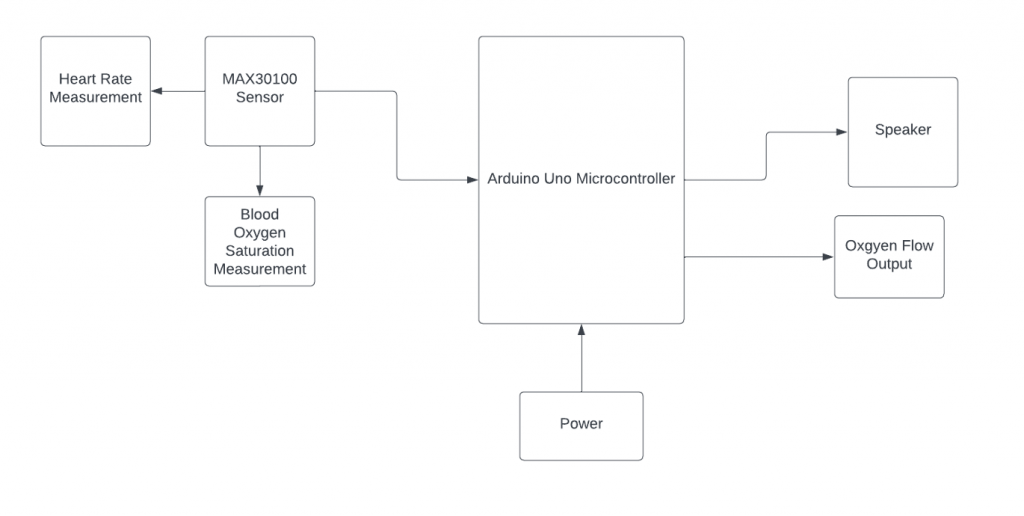
Figure 1. Control Process of the emergency oxygen device.
Figure 1 shows the control process of the emergency oxygen device. The MAX30100 provides raw data in the form of infrared and red lights in analog signals. They are then converted into digital signals and processed by the Arduino microcontroller. The raw data is then put through multiple algorithms within the Arduino Uno. The algorithms include moving average, low pass, Kalman filter, and wavelet transform. Various algorithms were implemented to improve the accu- racy of the MAX30100 sensor data in an emergency oxygen device designed with an Arduino Uno. The moving average filter was used to smooth out noisy data, and a low pass filter was used to remove high frequency noise. A Kalman filter was used to estimate the true value of the heart rate. At the same time, wavelet transform was applied to analyze the input signals and identify the signal’s relevant features. The results showed that the combination of these algorithms significantly improved the accuracy of the MAX30100 sensor data, allowing for a more precise measurement of the patient’s vital signs.
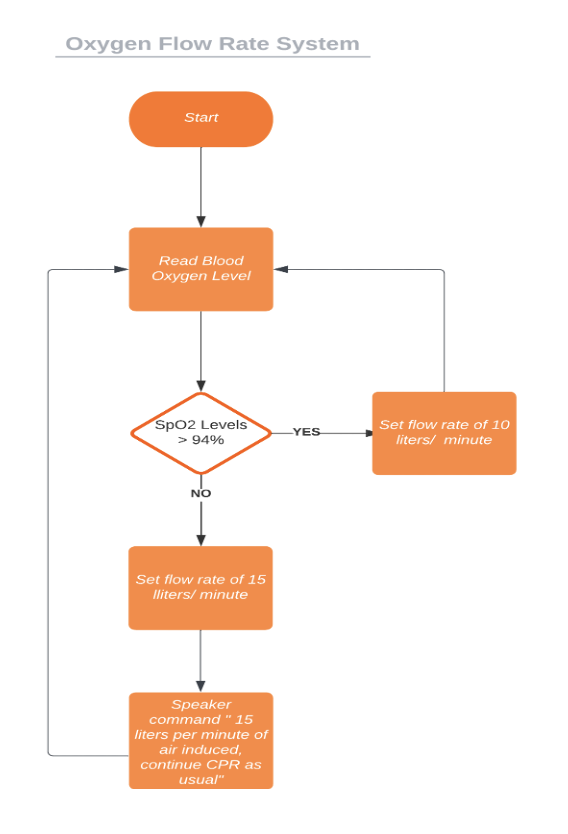
Figure 2. Oxygen flow rate system
The emergency oxygen device will operate based on the readings provided by the MAX30100 sensor, which will continuously monitor the victim’s blood oxygen level. If the blood oxygen level falls below 94%, the device will automatically dispense oxygen at a flow rate of 15 liters per minute to assist the victim in breathing. Conversely, if the oxygen level is above 94%, the flow rate will be reduced to 10 liters per minute to maintain a stable oxygen level. Figure 2 provides a visual to understand the flow process. In addition to providing oxygen, the device will guide users on how and when to give breaths to the victim through audio prompts. By using this device, it is expected that individuals with limited medical training will be able to provide immediate oxygen therapy to victims of respiratory distress in emergencies, potentially saving lives and improving patient outcomes. Figure 3 shows the device. On the top left hand, the diagram depicts the MAX30100 sensor connected to the Arduino Uno on the right hand. The bottom shows a pocket mask used for resuscitation and oxygen flow.
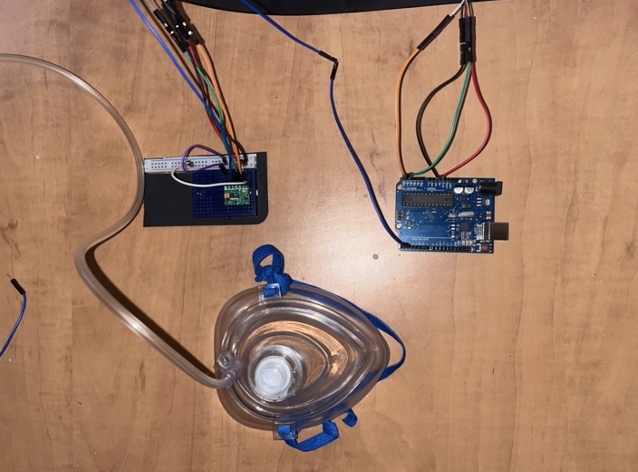
Figure 3. The device
Results
Table 1.
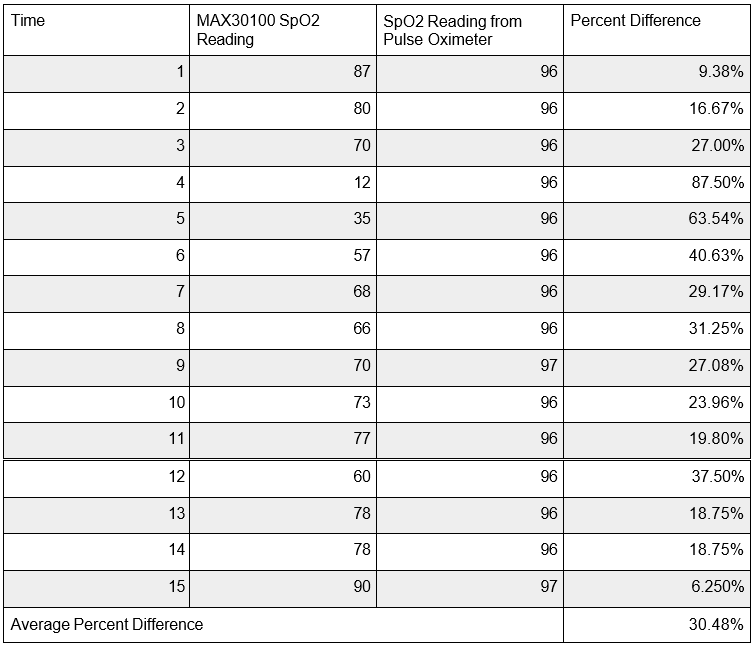
Table one displays the results of the MAX30100 sensor’s oxygen saturation level measurement without the use of filters and algorithms over a 15 second interval. The results show a maximum percent difference of 63.5% and a minimum of 6.25%. The average was 30.5%.
Table 2.
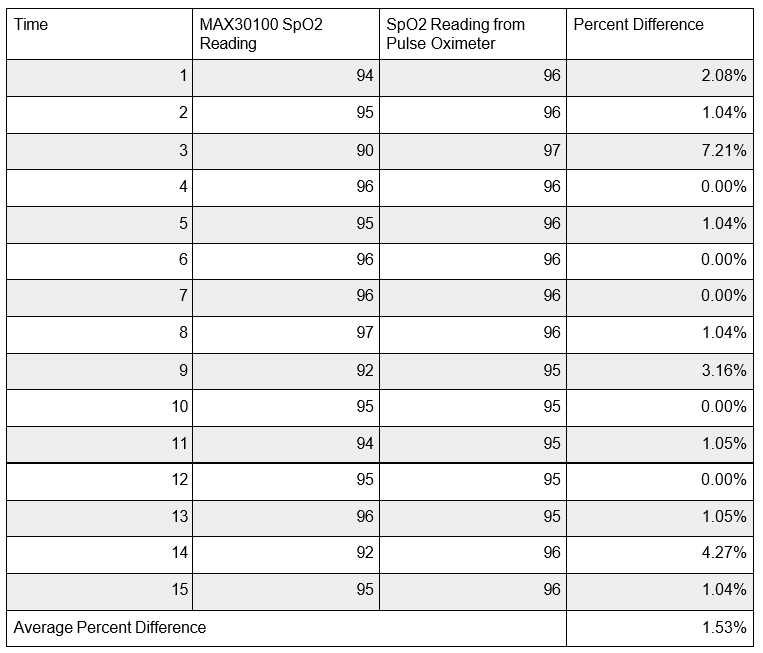
Table two shows the results of the MAX30100 sensor’s oxygen saturation level measurement with the use of filters and algorithms over a 15 second interval. The filters include, averaging filer, low pass filter, Kalman filter, and the wavelet transform algorithm. The results show a maximum per- cent difference of 7.21% and a minimum of 0.00%. The average was 1.53%. The average accuracy difference of the device over a 15.0 second interval changed from 30.5% to 1.53%.
Discussion
During the evaluation of the emergency oxygen device, it was found that the device initially had a low level of accuracy, showing data with an average percentage difference of up to 30.5%. However, after numerous data sets and various algorithms such as moving average, low pass, Kal-man filter, and wavelet transform, the device’s accuracy was significantly improved, with an aver- age percent difference of 1.53% compared to a pulse oximeter. Despite the significant improve- ment, the data sometimes still fluctuates, which indicates the need for further improvements in the device’s design and algorithm. The fluctuations can result from inaccuracy in the MAX30100 sen- sor and factors such as noise, lighting, temperature, humidity, skin colour, age, and gender, as it differs from each individual and the environment in which the tests were done. The data collected was only on one person, which lacked the demographic to provide more accurate data. Neverthe- less, the high level of accuracy achieved by the device makes it a promising solution for emergen- cies where victims require oxygen therapy.
This research paper presents an emergency
oxygen device based on the Max30100 sensor and Arduino Uno microcontroller, which provides oxygen therapy to patients in emergencies in which
oxygen might not be readily available. The device is designed to be portable,
quick, and easy to use. The device’s accuracy was evaluated, and it was found
that the device had a low level of accuracy
initially, showing data with inaccuracy. However, the device’s
accuracy was significantly improved after numerous
data sets and various algorithms. The data collected by the device was compared with an actual
pulse oximeter to determine this accuracy rate.
The device has advantages
over existing oxygen therapy devices, including its portability and ease of
use. The emergency oxygen device operates based on the readings provided by the MAX30100 sensor, which contin- uously
monitors the victim’s blood oxygen level. Overall, this device can
potentially improve the quality of care for patients in emergencies, and further studies
are needed to evaluate its effective-
ness in different clinical settings.
References
Bhuyan, Muhibul Haque, and Md Refat Sarder. “Design, Simulation, and Implementation of a Digital Pulse Oxygen Saturation Measurement System Using the Arduino Microcontroller.” In- ter-national Journal of Biomedical and Biological Engineering 15.2 (2021): 105-111.
Kane, Binita, Samantha Decalmer, and B. Ronan O’Driscoll. “Emergency oxygen therapy: from guideline to implementation.” Breathe 9.4 (2013): 246-253.
Reporter, S. R. H. D. (2020, July 17). Will CPR save your life? probably not, study says. WebMD. Retrieved September 13, 2022, from https://www.webmd.com/first- aid/news/20200717/will-cpr-save-your-life-probably-not-study-says
Singhal, Aneesh B. “A review of oxygen therapy in ischemic stroke.” Neurological research 29.2 (2007): 173-183.
William J. Mach, Amanda R, Thimmesch, Thomas Pierce J and Janet D. Pierce 2011 Conse- quences of Hyperoxia and the Toxicity of Oxygen in the Lung. Nursing Research and Practice. 20(11) 1-7. doi.org/10.1155/2011/260482
Young, Paul J., et al. “Conservative or liberal oxygen therapy in adults after cardiac arrest: an in- dividual-level patient data meta-analysis of randomised controlled trials.” Resuscitation 157 (2020): 15-22. Public access to automated external defibrillators (aed)s.
PUBLIC ACCESS TO AUTOMATED EXTERNAL DEFIBRILLATORS (AEDs). (2012, July).Retrieved September 14, 2022, from https://www.heartandstroke.ca/-/media/pdf-files/can- ada/other/pad-engfinal.ashx